CT-based clinical-radiomics model to predict progression and drive clinical applicability in locally advanced head and neck cancer
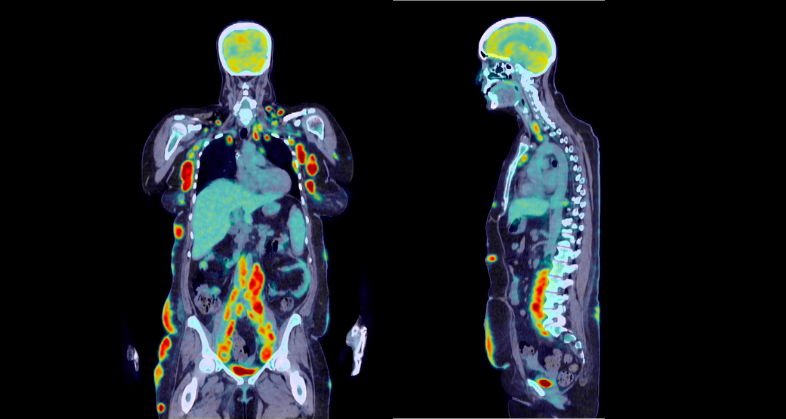
Imaging biomarkers from baseline CT scans for risk stratification of progression in locally advanced head and neck squamous cell carcinoma (LAHNSCC).
ApplicationOncology
The challenge
Definitive chemoradiation is currently the standard treatment for LAHNSCC. However, patient responses to the treatment vary, with some experiencing progression within five years of diagnosis. Consequently, there is a pressing need to stratify the risk of progression at diagnosis better, assisting clinicians in making informed treatment decisions. We aim to utilize imaging biomarkers derived from baseline CT scans to classify patients into high or low-risk progression categories.
The solution
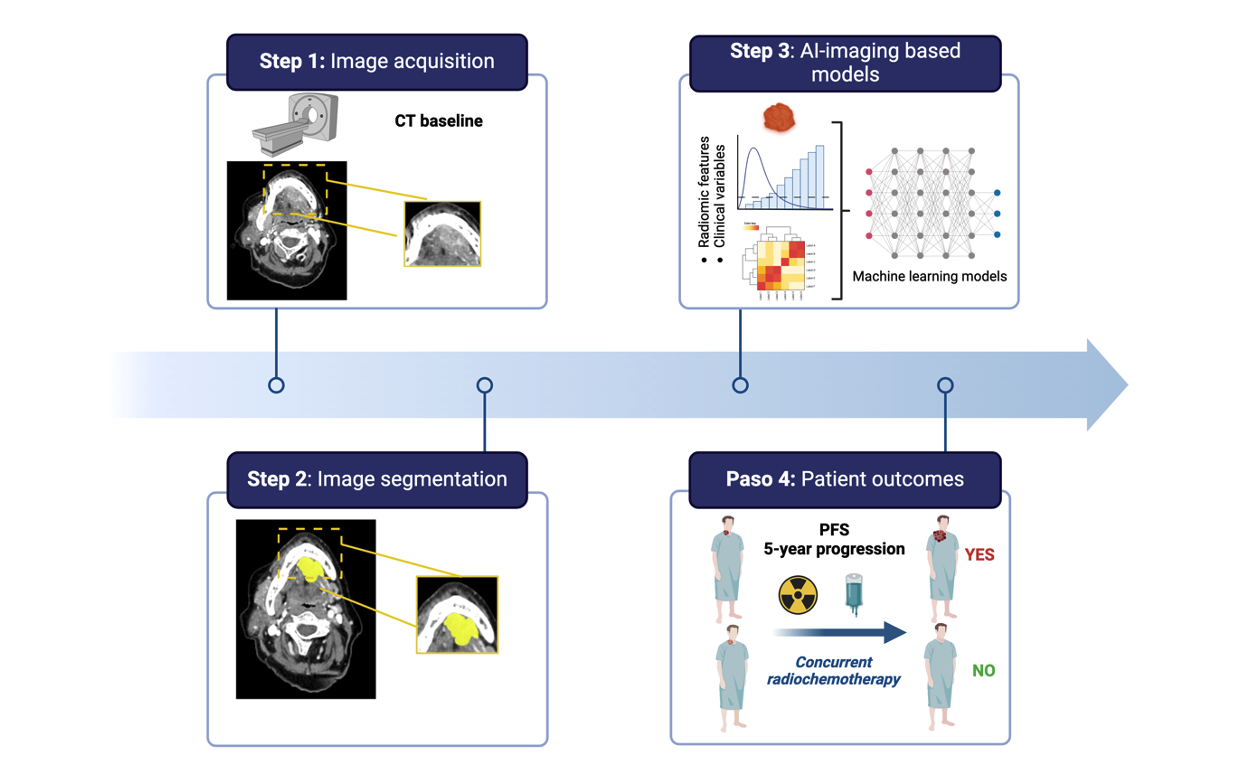
In a single-center, retrospective study, baseline CT scans and clinical data from 171 LAHNSCC patients treated with definitive chemoradiation were collected. Tumor segmentation was manually done by Quibim technicians using the Quibim platform under a radiologist’s supervision. Imaging biomarkers were extracted from each lesion, and the data underwent feature reduction. Following a 5-fold cross-validation, we tested several models for their predictive capacity for 5-year progression at diagnosis.
Figure 1. Radiomics workflow.
The outcome
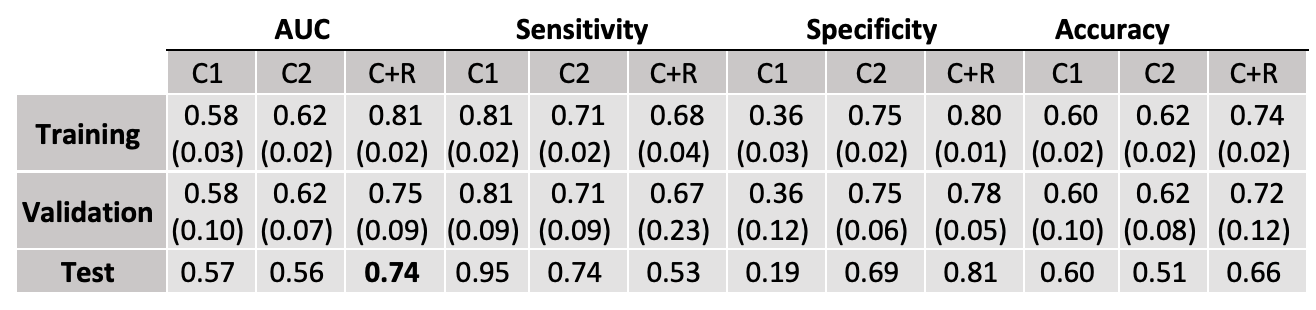
In our recently accepted publication in European Radiology, we demonstrate that the extreme gradient boosting model (XGBoost) most effectively predicted 5-year progression, including 12 radiomics features and four clinical variables (primary tumor site [oral cavity], TNM [tumor-nodes-metastasis], age, and smoking), achieving an AUC of 0.74, sensitivity of 0.53, specificity of 0.81 an accuracy of 0.66 on the test set, as shown in Table 1.
Table 1. Performance metrics obtained in 5-year progression prediction using TNM8 staging (C1), TNM8 and clinically significant variables (C2) and clinical and radiomics features (R+C) as input to the model, over training, validation and test subsets of data. Mean and standard deviation values across the 5-fold cross-validation process were calculated for training and validation values.
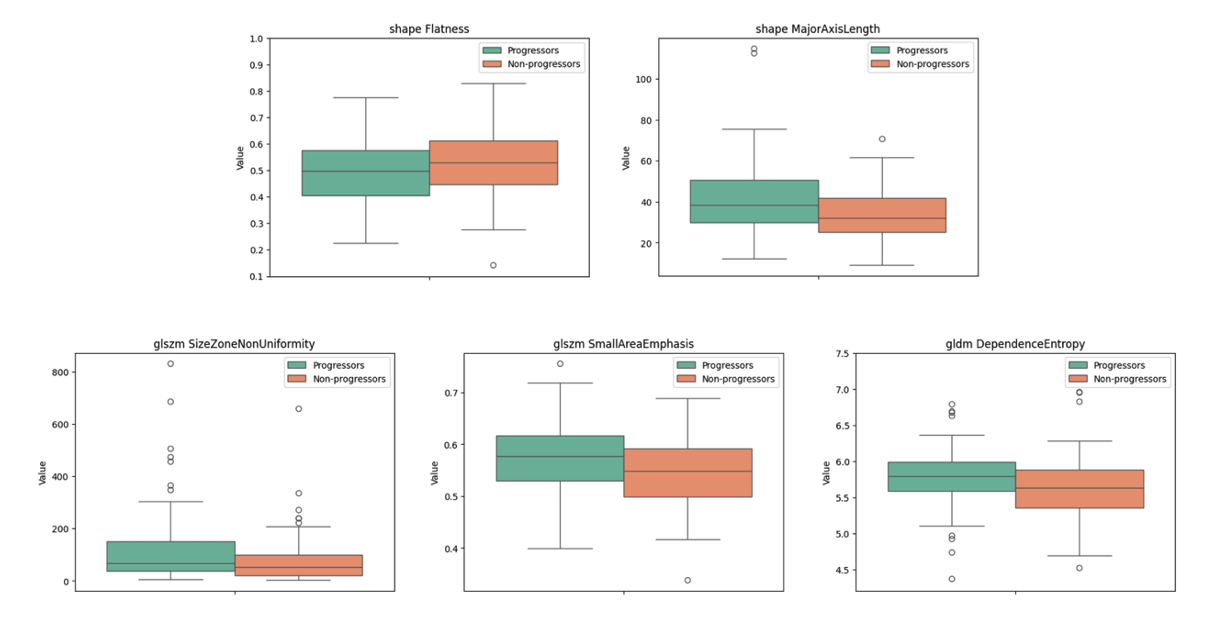
In addition, results obtained in the univariant analysis shows statistically significant differences between progressors and non-progressors in 5 radiomic variables. As displayed in Figure 2, the major axis length plot revealed that the largest diameter of the primary tumor was longer in progressors, while the second-order features revealed a more heterogeneous primary tumor in this same group.
Figure 2. Boxplot distributions of the radiomics features showing statistically significant differences between 5-year progression and no-progression patients. Shape Flatness (p-value 0.028), Shape Major axis length (p-value 0.006), Second order GLSZM Size zone non-uniformity (p-value 0.020), Second order GLSZM Small area emphasis (p-value 0.016) and Second order GLDM Dependence entropy (p-value 0.037). Abbreviations: GLRLM (Gray-Level Run Length Matrix), GLSZM (Gray-Level Size Zone Matrix), GLDM (Gray-Level Dependence Matrix.
In conclusion, a comprehensive model for LAHNSCC based on CT-radiomics features and including routine clinical variables shows remarkable accuracy in stratifying risk groups, outperforming current clinical models. However, prospective external validation is required to confirm these findings.
Reference:
Bruixola, G., Dualde-Beltrán, D., Jimenez-Pastor, A., Nogué, A., Bellvís, F., Fuster-Matanzo, A., Alfaro-Cervelló, C., Grimalt, N., Salhab-Ibáñez, N., Escorihuela, V., Iglesias, M. E., Maroñas, M., Alberich-Bayarri, Á., Cervantes, A., & Tarazona, N. (in press). CT-based clinical-radiomics model to predict progression and drive clinical applicability in locally advanced head and neck cancer. European Radiology.
Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam, quis nostrud exercitation ullamco laboris nisi ut aliquip ex ea commodo consequat.